1 The Trillion-Dollar Question
Between August 2024 and August 2025, Novo Nordisk lost roughly two-thirds of its market value from all-time highs. Gone. Nearly everything the GLP-1 expansion built, wiped out in twelve months. Over that same stretch, Eli Lilly's stock climbed about 40% and the company crossed the trillion-dollar mark - a first for any pharma name. By late summer, Lilly was valued at roughly four times Novo's market cap. And here's what kept nagging at me: Lilly was producing only modestly higher net income, and at times, lower operating cash flow.
I spent three hours with both companies' financials going back three years. Couldn't reconcile the gap. Whatever setbacks Novo endured, whatever edge Lilly gained, the actual numbers - revenues, margins, balance sheets - don't justify a trillion-dollar company staring across at a two-hundred-billion-dollar one. Not even close.
The market, I think, confused Novo's temporary stumbles with permanent damage. That slide below $50 wasn't driven by business fundamentals falling apart. It was narrative. Psychology. Momentum feeding on itself. The real question isn't which company "wins" a single quarter's headline. It's whether both remain essential to the largest chronic disease market in history. They do. And one of them is dramatically mispriced.
2 Semaglutide: The Drug That Built an Empire - and Then Nearly Destroyed Its Creator's Stock
How does a pharma company growing revenues at 18% a year, selling what might be the most consequential prescription drug on the planet, lose 65% of its stock price in twelve months? To answer that, you need to understand what semaglutide actually is. And what it's done.
Semaglutide is a GLP-1 receptor agonist approved for type 2 diabetes (Ozempic, December 2017) and obesity (Wegovy, June 2021). Before it arrived, the scientific community genuinely did not believe pharmacology could deliver 15–20%+ weight loss. The mechanism - stimulating insulin release, reducing glucagon, slowing gastric emptying, suppressing appetite - turned out to be groundbreaking. That word gets overused in pharma. Here it's earned.
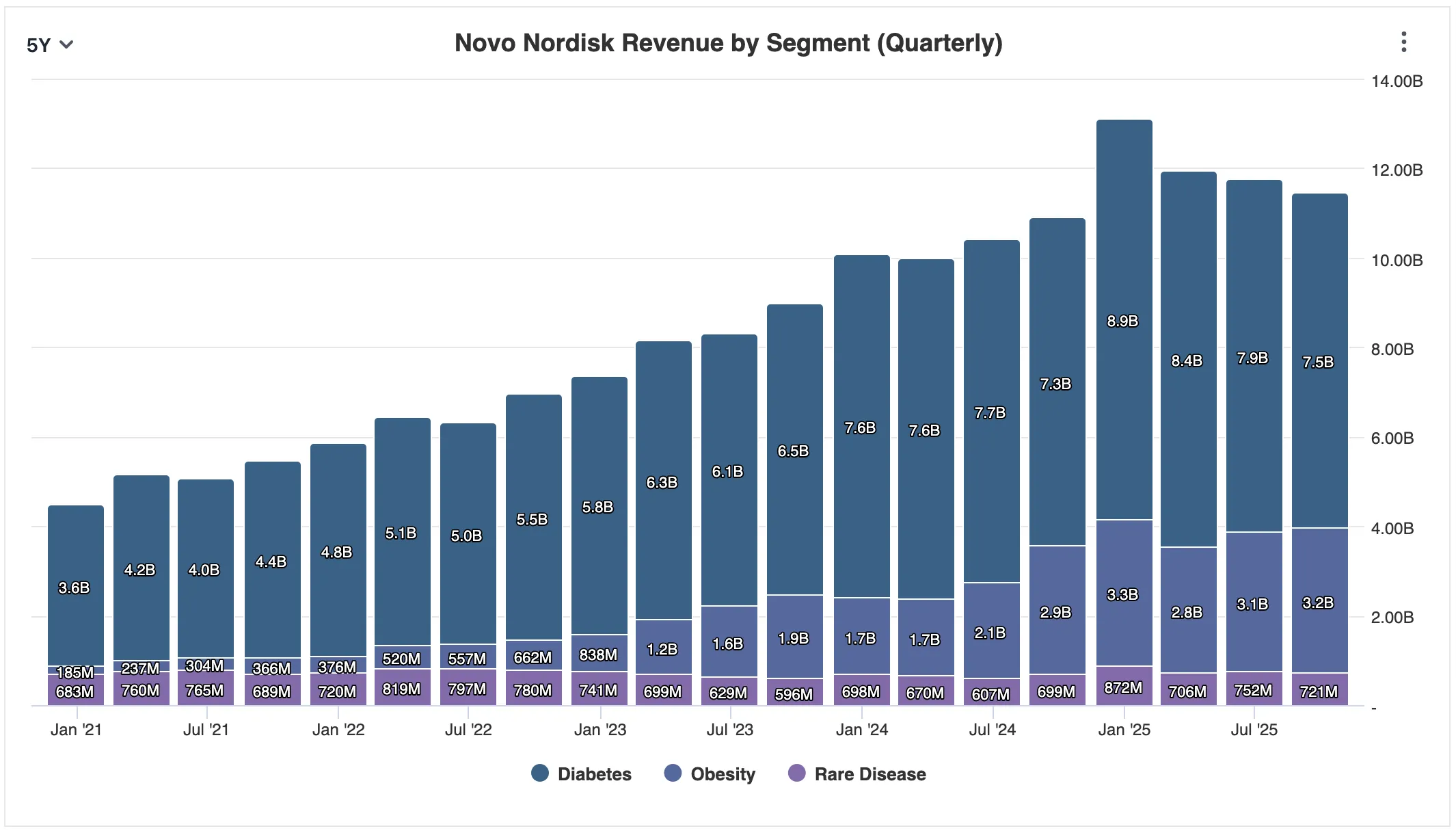
The commercial numbers tell the rest of the story. Ozempic brought in roughly $8.3 billion in 2022. Wegovy added $860 million. Fast forward to 2025, and based on Q3 performance, Ozempic is tracking toward approximately $19.6 billion annually while Wegovy is heading for $11.8 billion. Together that's about 66% of Novo's estimated $48 billion in total revenue. Wegovy sales up 45% year-over-year. Ozempic up 17%. Analysts see a path to $60 billion in peak annual revenues by 2031.
Yes, Novo is heavily concentrated. The diabetes and obesity segments generated $10.7 billion in Q3 alone - dwarfing the $0.72 billion from rare diseases. Is that concentration a strength or a vulnerability? Both, obviously. But the market semaglutide serves is large enough - and growing fast enough - that the concentration looks more like focus than fragility.
So - crisis, what crisis? How does a company on this trajectory lose two-thirds of its market value? A collision of real setbacks and narrative that fed on itself.
The underwhelming Phase III data for CagriSema hit first - Novo's next-gen triple agonist that management had promised would deliver 25%+ weight loss. Then Trump-era tariff threats against pharma imports. Then the departure of longstanding CEO Lars Fruergaard Jørgensen in May 2025. And threading through all of it, the relentless advance of Eli Lilly and tirzepatide (Mounjaro/Zepbound) providing a clean counter-narrative: Lilly was winning, Novo was finished. Simple story. Easy to trade on.
That's how modern U.S. equity markets work now, especially with retail participation driving narrative momentum. Valuation spreads between "winners" and "disappointments" don't just widen - they overshoot in both directions. Lilly became a symbol stock. Headlines of explosive growth and uninterrupted price action reinforced each other in a loop. Capital didn't reallocate. It crowded. Temporary setbacks started looking permanent. And momentum begat momentum.
3 Novo Is Not a U.S.-Only Story - and the Market Priced It as If It Were
Most of the Novo-versus-Lilly narrative these past two years has been filtered through a U.S. lens. Declining American market share. Regulatory headaches from Washington. Pricing pressure from compounders exploiting loopholes through platforms like Hims & Hers. Fair enough - the U.S. is the most profitable pharma market on earth.
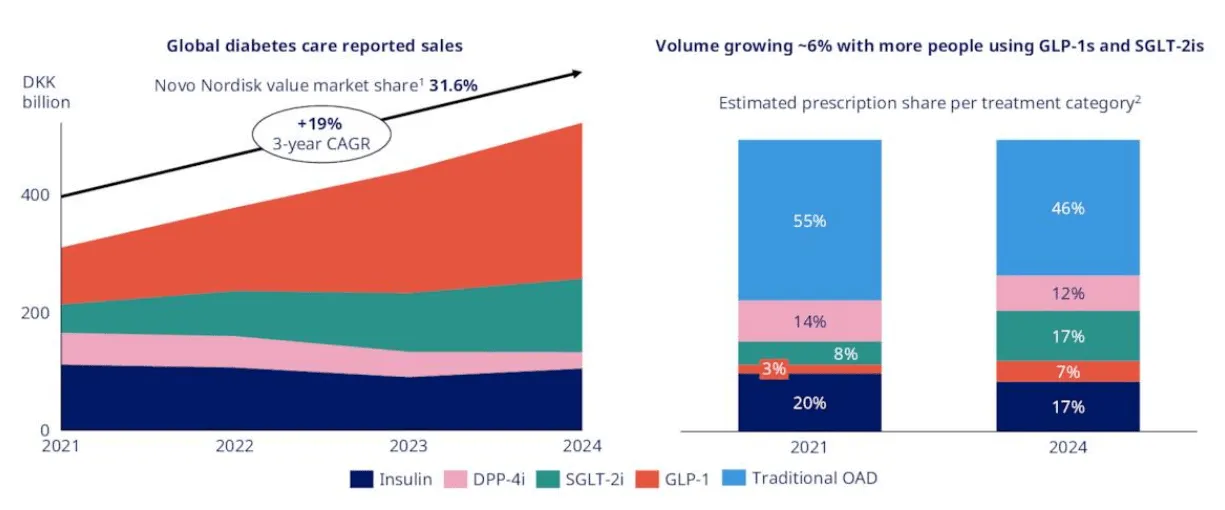
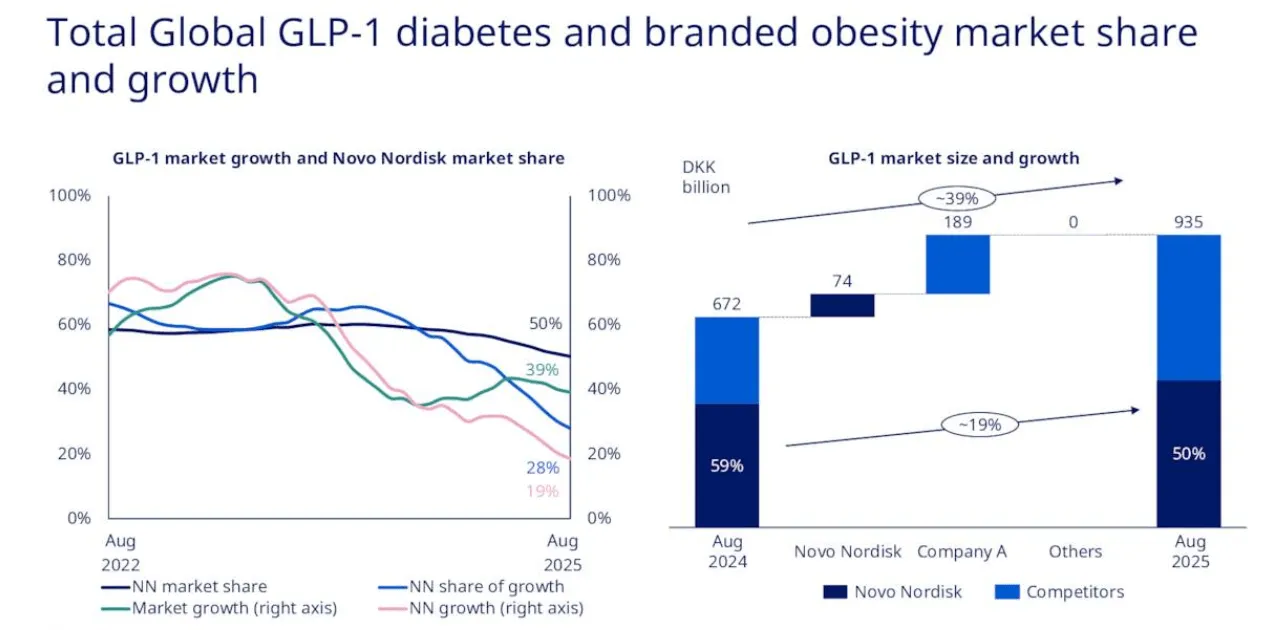
But here's the thing. The U.S. accounts for roughly half of Novo's revenue and about two-thirds of Lilly's. Novo might be the least U.S.-dependent major pharma company in existence. Long before GLP-1 drugs became headlines, Novo spent decades building dominant insulin and diabetes franchises across Europe, Latin America, the Middle East, and Asia. In many of those markets, they're the institutional default - top of the short list for public health systems, national formularies, hospital networks. Their 2024 annual report puts it plainly: "the global market leader in the GLP-1 segment with a 55.1% value market share" and "the global market leader with a volume market share of 70.4% of the branded obesity market."
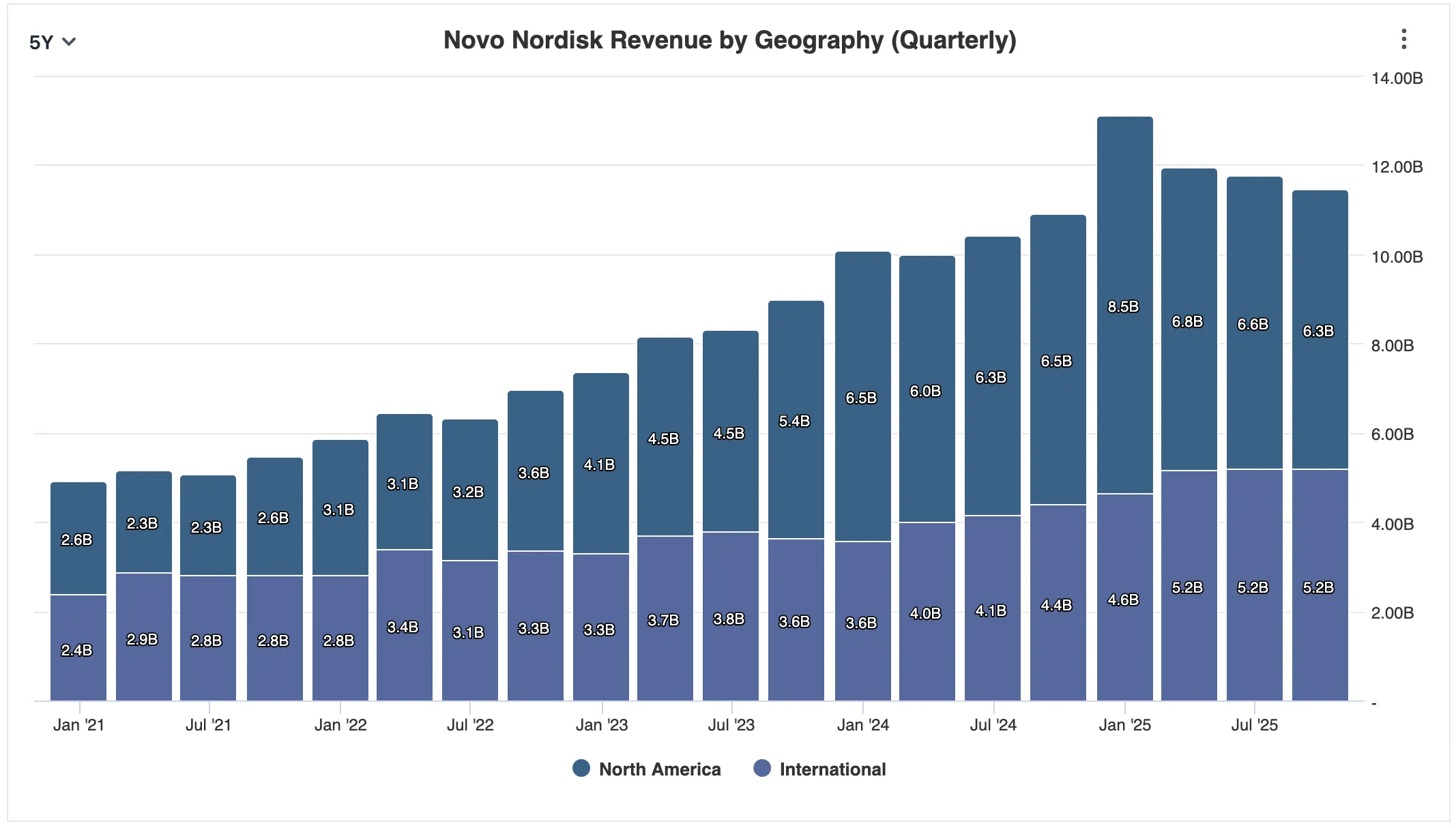
Q3 alone: international revenue topped $5.2 billion against $6.3 billion from the U.S. In previous years, ex-US revenue ran nearly equal to domestic. Past two years that shifted - reflecting the Ozempic and Wegovy success in America. But obesity pharmacotherapy isn't spreading only through compounders and social media in the U.S. It's spreading through health systems globally. And 95% of the world's population lives outside the United States. Novo has been cultivating those relationships for decades.
At January's JPMorgan Healthcare Conference, new CEO Maziar Doustdar hammered this point. He framed Novo not as a U.S.-centric drug company but as a global metabolic franchise serving nearly two billion people worldwide. Outside the U.S., prescription penetration is still extremely low. America may be in the first inning. Most of the world hasn't come to bat yet.
But when investors decided Lilly was "winning" based largely on U.S. data, Novo got punished as if global metabolic markets were either irrelevant or already decided. Think about what that assumes. That Novo's manufacturing prowess, regulatory expertise across dozens of jurisdictions, and distribution networks built over a hundred years barely matter. Try sustaining that conclusion when you actually look at the numbers.
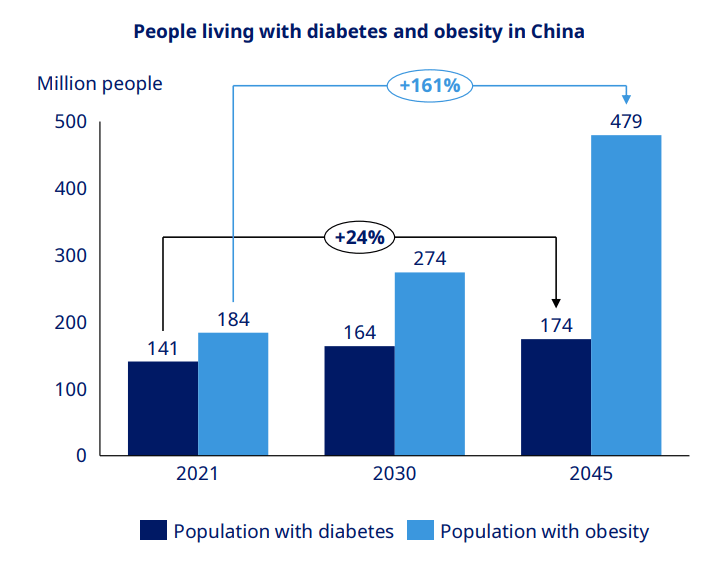
China alone tells a striking story. Novo holds near-80% market share for GLP-1 agonists there. TTM revenue from the region: approximately $2.96 billion, about 6% of the total. Yes, generic competition is intensifying - 15 to 16 Chinese companies are developing semaglutide equivalents, and Novo recently slashed injectable Wegovy prices across Chinese provinces by up to 50%. But step back. The market is enormous (148 million adults with diabetes, potentially 65% of the population overweight or obese by 2030) and still fundamentally in its infancy. This isn't about defending a shrinking pie. The pie is barely out of the oven.
4 The Oral Pill Changes the Competitive Psychology
For a year, the central knock on Novo was simple: Lilly was winning the injectable race. Tirzepatide's marginally better weight loss numbers (20–22% versus semaglutide's 15–17%) looked like an enduring edge. The whole debate had narrowed to injectable trial percentages, as if obesity pharmacotherapy were a one-dimensional sprint.
Then December 22, 2025. The FDA approved Novo's oral Wegovy - the first FDA-approved oral GLP-1 treatment for obesity. OASIS-4 showed 25 mg of oral semaglutide taken daily reduced weight by 16.6% on average, with one in three patients hitting 20% or greater weight loss. Over 3,000 patients in the first week. More than 18,000 prescriptions in the first full week of availability. That's not a soft launch.
And this isn't just a new formulation. It changes the game entirely. Injectables capture a specific patient: highly motivated, insured, medically engaged. A pill opens the door to everyone else. Billions of overweight or obese people worldwide will never self-inject unless a doctor practically begs them. Oral therapy normalizes weight-loss treatment - moves it closer to statins, to blood pressure meds. Routine medication. No stigma, no needles.
OASIS-4 Weight Loss
Pivotal Trial Weight Loss
Then there's refrigeration. Injectable Wegovy and Zepbound need cold-chain storage. A pill doesn't. If you travel, live in a rural area, or just find weekly injection logistics annoying, that difference is material. It's not a minor convenience upgrade - it's the kind of thing that determines whether patients actually stick with treatment.
Doustdar made this visceral at JPMorgan. His father-in-law wanted a GLP-1 treatment but flat-out refused to inject. A friend in Montana wanted to switch off Lilly's injectable because he was "simply too nervous about keeping the medication in cold chain" while traveling. These aren't edge cases. They're the vast middle of the addressable market that injectables alone will never reach.
Meanwhile, Lilly's oral candidate orforglipron has had its FDA decision pushed to April 10th. Pivotal data showed mean weight loss of 7.9% - respectable, sure, but roughly half of oral Wegovy's 16.6%. Tolerability is also weaker: approximately 22–24% of patients at the highest orforglipron dose dropped out due to adverse events, versus just 7% for oral Wegovy. That's a three-to-one discontinuation gap.
The Dosing Controversy: What Lilly's Head-to-Head Trial Actually Shows
In September, Lilly published a head-to-head trial: oral semaglutide (7 mg and 14 mg) versus orforglipron (12 mg and 36 mg). Surface read? Orforglipron outperformed on blood sugar control and weight loss. But there's a problem buried in the trial design: the semaglutide doses Lilly chose (7 mg and 14 mg) were significantly lower than the 25 mg dose Novo used in its pivotal OASIS-4 trial.
That's like testing England's reserve squad against Spain's starting eleven and declaring Spain the better team. Why didn't Lilly trial orforglipron against the 25 mg dose Novo has used since 2023? They cited "approved label instructions," but earlier Lancet-published studies had already established 25 mg and 50 mg as the clinically relevant doses. Novo's CEO at JPMorgan, with pointed understatement: "The world, in my opinion, has a little bit misread this."
ATTAIN-MAINTAIN, published early January, piled on. Patients switching from Zepbound to orforglipron gained back 5 kg - roughly 20% of their original weight loss - versus just 0.9 kg for those switching from Wegovy. Discontinuation rates ran higher too (7.2% vs 4.8%). That data suggests orforglipron may be an inferior product to the very injectable it's supposed to replace.
5 Airbus vs. Boeing: The Right Framework for This Rivalry
Wall Street keeps framing this as a duel. One wins, one loses. That framing is wrong. This is a duopoly. It'll play out over decades, not quarters.
Think about Airbus and Boeing. Each has suffered execution crises, regulatory nightmares, public embarrassment. Each has won some cycles and lost others. Neither disappeared. The structure of global commercial aviation simply does not permit a single supplier. No airline, no government, no regulator will hand their entire fleet to one manufacturer. It would be insane.
Cardiometabolic medicine works the same way. No government, insurer, or health system will entrust all its obesity and diabetes care to one company. Pricing leverage, supply chain risk, geopolitics - everything conspires to guarantee a multi-supplier market. So the investment question isn't who captures the next headline. It's whether both remain essential, and which one offers the better entry point right now.
Buying Boeing below $150 during the 737 MAX crisis didn't require believing Boeing would dominate Airbus. It required believing Boeing would remain indispensable - and solvent. That was enough. Same logic applies to Novo below $50. You didn't need to believe Novo would defeat Lilly. You needed to believe it would remain one of two foundational suppliers to one of the largest chronic disease markets in history. Solvency? Never in doubt.
Where the Analogy Breaks: Generics and Patent Cliffs
One critical difference, though. Nobody has ever seen a generic Boeing 747. But the world will soon see generic GLP-1 drugs. Dr. Reddy's already won Indian approval for a generic Ozempic. Fifteen Chinese companies are developing semaglutide equivalents. Patent cliffs are the inescapable long-term risk for both companies, and they mean this duopoly probably won't last as long as Boeing/Airbus. Which is exactly why valuation discipline matters - and why Novo's current discount to Lilly is significant.
6 The New CEO: A Commercial Operator With Something to Prove
In August 2025, Novo tapped Maziar "Mike" Doustdar as CEO. Company lifer. Joined in 1992 as an office clerk in Vienna, worked his way up to running the entire international business. Under his watch, international operations grew into a franchise generating well over $15 billion annually. Not a scientist. A commercial operator. That distinction matters - more on it below.
His JPMorgan fireside chat in January might end up being the most consequential pharma CEO interview of 2026. Three things jumped out at me:
First, he narrowed the focus. Previous management chased adjacencies and over-promised on CagriSema. Doustdar was blunt: Novo's core is diabetes and obesity, full stop, and that core serves two billion people. "Those couple of things have 2 billion people suffering from those conditions. We are only touching the surface when it comes to treatment of these individuals." Translation: stop worrying about what Novo doesn't do. Focus on what it does better than anyone.
Second, he admitted mistakes. When does a CEO at a $200 billion company do that? He was candid about Novo's failure to understand U.S. insurance realities - the gap between theoretical coverage (55 million insured patients) and the actual maze of pre-authorizations and access barriers. Announced partnerships with Ro, LifeMD, Amazon, WeightWatchers, and Costco to build direct-to-consumer channels. "Us and Lilly combined have probably 10 million, 15 million patients. What about the other 85 million? We need to get to them."
Third, he went after Lilly directly. On tolerability: "Some 7% of our trial participants left due to tolerability issues. When you look at my competitors, it was around 22% to 24% at the highest dose." On dosing: "Our company is a bit conservative when it comes to these things… when you are second to market and you're designing your trials, you tell yourself, I've got to go all the way up to 15 milligrams to get there." The subtext wasn't even sub at that point. Lilly got its headline weight-loss numbers by pushing dosing higher. Novo took a more conservative path and still delivered a superior oral product.
The Leadership Risk
Doustdar is a capable commercial operator. No question. But his background is international business, not science. And drug companies aren't consumer goods companies - they're long-cycle research organizations where the most consequential decisions involve allocating capital across uncertain clinical programs. A CEO with a scientific background carries a long-term edge in Big Pharma. That doesn't disqualify Doustdar (plenty of successful pharma CEOs weren't scientists), but it puts more weight on the strength and independence of Novo's R&D leadership. The board needs to make sure the science doesn't become subordinate to commercial instinct.
7 Manufacturing: The Race Within the Race
Efficacy matters. But in 2025–2026? The winner might simply be whoever can produce the most doses. Both companies are in the middle of the largest manufacturing buildout pharma has ever seen - collectively committing over $43 billion in capital expenditure. That's not a typo.
Novo Nordisk - $25B+ CapEx
- Kalundborg 2.0 (Denmark) - $6.5B, 2.5x current output, phased 2024–2027
- Chartres (France) - $2.9B, fill-finish +150%, Q3 2026
- Clayton (North Carolina) - $4.1B, US production base, 2026–2029
- Odense (Denmark) - $1.8B, oral semaglutide focus, late 2025
- Montes Claros (Brazil) - $320M, Latin America supply, Q2 2026
Capacity increase: 3–4x by 2027
Eli Lilly - $18B+ CapEx
- Lebanon Gigafactory (Indiana) - $3.7B, injectable biologics, 2025–2028
- LEAP Innovation (Indiana) - $4.5B, modular pods, 2026–2030
- Concord (North Carolina) - $800M, oral GLP-1, Q4 2025
- Limerick (Ireland) - $1.8B, Europe API, 2026–2027
- Alzey Acquisition (Germany) - $2.7B, instant capacity, 2025
Capacity increase: 5–6x by 2027
Lilly arguably leads on capacity growth rate - the modular LEAP facility design and instant capacity from the Boehringer Ingelheim acquisition give them a head start. But in a post-tariff world, concentrating $27 billion of manufacturing in the U.S. could backfire if trade dynamics shift. Novo's footprint is more scattered - Denmark, France, Brazil - and that geographic diversification might prove strategically valuable in ways nobody's pricing in yet. Plus Novo's Odense expansion targets oral semaglutide specifically, giving it an uncontested supply advantage in a product category where Lilly has nothing approved.
8 The Numbers That Matter: Why Novo Looks Mispriced
The balance sheet is clean. $5.02 billion in cash and equivalents, $28.03 billion in current assets, $78.94 billion total. Debt sits at $15.59 billion, but only $1.85 billion comes due in the next 12 months - easily covered when you're throwing off $5.0 billion in quarterly free cash flow ($10.17 billion trailing twelve months). Debt-to-equity of 0.6. Comfortable. And shareholders get paid: dividends plus buybacks yield 3.75%.
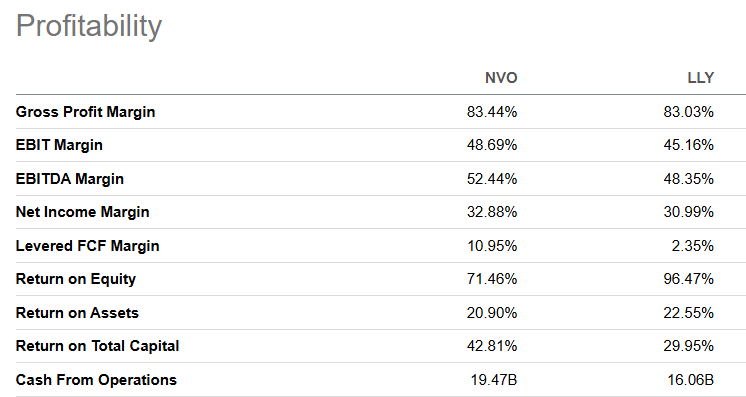
Profitability: NVO vs LLY
Here's what makes the valuation gap genuinely puzzling. Novo isn't just competitive with Lilly on profitability - it's superior on most metrics:
| Metric | NVO | LLY |
|---|---|---|
| Gross Profit Margin | 83.44% | 83.03% |
| EBIT Margin | 48.69% | 45.16% |
| EBITDA Margin | 52.44% | 48.35% |
| Net Income Margin | 32.88% | 30.99% |
| Levered FCF Margin | 10.95% | 2.35% |
| Return on Equity | 71.46% | 96.47% |
| Return on Assets | 20.90% | 22.55% |
| Return on Total Capital | 42.81% | 29.95% |
| Cash From Operations | $19.47B | $16.06B |
The Valuation Disconnect
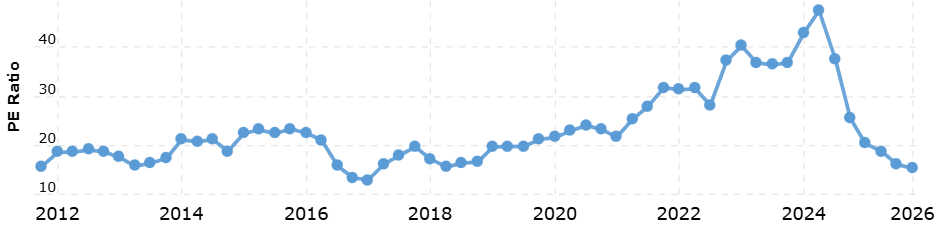
And yet. Novo trades at roughly 17x earnings. Lilly at 51x. On price-to-sales, Novo sits at about 5.6x versus Lilly's 16x. Novo's P/E is at its lowest in seven or eight years - one of the lowest in the company's history. So is this a value trap?
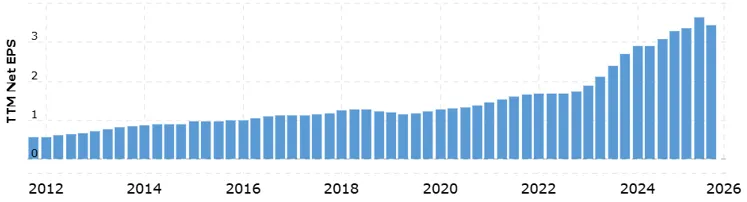
Look at the EPS chart. Fourteen years of consistent growth, with recent acceleration from the GLP-1 franchise. Value trap? Extremely unlikely. The earnings trajectory hasn't broken. What broke was sentiment.
Yes, Lilly has broader product diversity - Kisunla for Alzheimer's adds real revenue diversification. But let's be honest about what's actually driven Lilly's 400%+ share price gains over five years. It's tirzepatide. A drug that is far more similar to semaglutide than it is different from it. For the market to slap a 3x valuation premium on one company over the other - when both run on the same drug class, serve the same patients, post comparable margins - that requires extraordinary conviction that one will permanently dominate and the other permanently decline. I don't see evidence for that conviction. Not in the clinical data, not in the financials, not anywhere.
9 Catalysts, Risks, and What Could Go Wrong
Key Risks for Both Companies
Short-term: Novo's stock has already partially priced in oral Wegovy and strong early sales. Any disappointment in rollout pace or Q4 earnings sends shares right back down. On Lilly's side, the orforglipron delay to April creates overhang - and at current valuations, weaker-than-expected data gets punished hard.
Intermediate-term: Pricing pressure is coming. Both companies agreed to drop U.S. prices from ~$1,300/month to ~$350 via the Trump Administration's pricing deals. Manufacturing may strain. Competition intensifies - Amgen, Roche, Viking Therapeutics, multiple Chinese companies, all chasing GLP-1 opportunities. Some of them will succeed.
Long-term: Patent cliffs. The inescapable risk for both. Blockbuster GLP-1 drugs will face generic competition - that's a when, not an if. Dr. Reddy's already has Indian approval for generic Ozempic. This isn't theoretical. It's imminent.
Emerging Challengers Worth Monitoring
Amgen (Maritide): Monthly dosing GLP-1/GIP dual agonist. 14.5% weight loss at 12 weeks in Phase 2, potential 2027 approval. Viking Therapeutics (VK2735): 15.7% weight loss at 13 weeks - but frankly, more likely an acquisition target than an independent competitor. Pfizer (Danuglipron): Discontinued October 2025 after 40%+ adverse event dropouts. A useful reminder that oral GLP-1 development is genuinely hard, which makes what Novo pulled off with oral Wegovy look even more impressive.
Even so, the duopoly likely holds 80%+ combined market share through at least 2028. New entrants lack the 4–7 years needed to build GLP-1 manufacturing at scale. And comprehensive patent estates provide protection through the early 2030s.
10 Conclusion: Two Companies, Two Prices, One Market
Here is what we know. A 103-year-old company that essentially created the global market for metabolic disease treatment is trading like its best days are behind it. Meanwhile, a company whose recent success rides almost entirely on a drug class that Novo pioneered is priced for perfection over the next decade.
The clinical data doesn't support the "Lilly won" narrative. Oral Wegovy looks like the superior oral product by a wide margin. ATTAIN-MAINTAIN raises real questions about orforglipron's ability to retain patients switching from Zepbound. And Novo's global infrastructure - particularly outside the U.S. - provides growth levers that American-focused analysts keep underweighting.
To be clear: this is not a "sell Lilly, buy Novo" call. Lilly remains formidable - diversified pipeline, faster-growing manufacturing capacity, strong U.S. execution. What I'm saying is that the market has mispriced the relative positioning. The narrative simplified a complex rivalry into "Lilly wins." Reality is messier than that.
"Luckily, in the obesity space, it is not the case that you must buy Novo and sell Lilly, or sell Novo and buy Lilly. You can own both, and they may even be good for one another, as Pepsi's rivalry with Coke is arguably good for both companies. Under its new CEO, Novo is taking the fight to Lilly in a way it was unable to do last year. The world, in our opinion, has a little bit misread how to value Novo Nordisk's business - but we expect this to change in 2026."
- Bellwether Research, Research TeamLet me make the argument specific and falsifiable. The market is pricing Novo as structurally impaired - implying near-zero long-term growth in a reverse-DCF framework - while pricing Lilly as if tirzepatide's U.S. dominance is permanent and uncontested. A 17x-versus-51x earnings gap between two companies with comparable margins, in the same drug class, serving the same global patient population, is not a measured judgment. It's an overreaction. Duopolies don't require one competitor to collapse for the other to thrive. Airbus didn't need Boeing to disappear. Pepsi doesn't need Coke to go bankrupt. The convergence trade here isn't about Novo "winning." It's about the market recognizing that it doesn't need to.
The Boeing/Airbus analogy does break at one critical point, though - and it's worth being honest about where. Boeing's crises were reputational and regulatory. Novo's problem is operational: it can't yet produce enough doses to satisfy global demand. Different risk categories entirely. If the problem were a moat problem - a competitor's drug genuinely superior across every dimension - that would be structural and slow to fix. But a manufacturing problem has a known resolution: capital expenditure, time, execution. Novo has committed the capital. The risk is timeline and execution, not obsolescence.
Two things would weaken this thesis materially. First: semaglutide losing U.S. formulary position faster than current trends suggest, driven by Lilly's aggressive PBM contracting or orforglipron's commercial launch surprising to the upside. Second: Lilly's SURPASS-CVOT data demonstrating tirzepatide superiority in cardiovascular outcomes - extending the clinical edge beyond obesity into cardiology, where Novo's SELECT trial currently holds the stronger evidence base. Either development shifts the duopoly calculus away from parity.
What to watch is narrow. Novo's quarterly manufacturing capacity additions versus its own stated targets. And U.S. formulary access negotiations for 2026 - specifically whether oral Wegovy secures preferred tier placement against orforglipron. If capacity scales on schedule and formulary position holds, the valuation gap has no durable justification. Full stop.
Investment Disclaimer
This article is for educational and analytical purposes only and does not constitute financial or medical advice. Pharmaceutical investments carry significant risks including clinical trial failures, regulatory delays, patent challenges, and manufacturing setbacks. GLP-1 drugs have known side effects and long-term safety data is still being collected.
Market projections are estimates based on consensus data and may differ materially from actual results. Medicare coverage, competitive dynamics, and pricing pressures could significantly impact forecasts. Consider consulting a financial advisor before making investment decisions based on this analysis.
Bellwether Research, Market Research, January 23, 2026